How Cerebral Is Improving Response Times to Help Patients in Crisis


Blog Authors: Ivan Lopez, Akshay Swaminathan, Rafael Antonio Garcia Mar, Tom McClintock
Upon calling any medical provider, the first thing you typically hear is: “If this is an emergency, please hang up and call 911.” Though these words are extremely common, little is known about the “standard” care journey for patients experiencing a mental health emergency.
Sadly, most mental health providers do not track the number of patients who call experiencing a crisis. For patients who end up calling 911, there is little data shared about the average wait times they experience before their emergencies are addressed.
To help address these gaps, Cerebral has developed a data-driven approach to improve clinical safety, especially as it relates to mental health emergencies. On a typical day, Cerebral receives 5,000-10,000 patient messages via a chat system available on our website or mobile application. This allows patients to connect with their care team on a variety of topics such as appointment rescheduling, questions about their treatment plans, medications, and more. It also serves as a form of contact for patients who are experiencing a crisis.

Each patient message is reviewed and addressed by our patient support team. While this approach is best suited for non-emergencies, more serious mental health crises, such as suicidal ideation (when someone is having suicidal thoughts or ideas), need to be addressed and responded to as soon as possible. With this as our guide, we’ve developed ways to improve our response time in emergency cases.
Using machine learning-enabled tools to improve mental healthcare delivery
Machine learning (ML) and artificial intelligence (AI) are critical tools in the advancement of mental health care, but these benefits are only possible at scale. Both technologies require many data points to test and validate hypotheses in order to prove that the systems are working effectively. Because of Cerebral’s experience serving a quarter-million people (and counting), we are uniquely suited to develop and implement cutting edge ML/AI tools to supplement the expertise of our clinicians and help improve clinical outcomes. This means we can make sure our patients are safe around the clock and get them the help they need as quickly as possible. While all messages are and will continue to be viewed by Cerebral's professional staff, our innovative ML/AI tool allows our teams the ability to respond to patients in crisis in near real-time.
With the help of a team of clinicians, crisis specialists and data scientists, we analyzed millions of patient messages to build a tool that would detect any indication of crisis. We call this tool the Crisis Message Detector 1 (CMD-1).
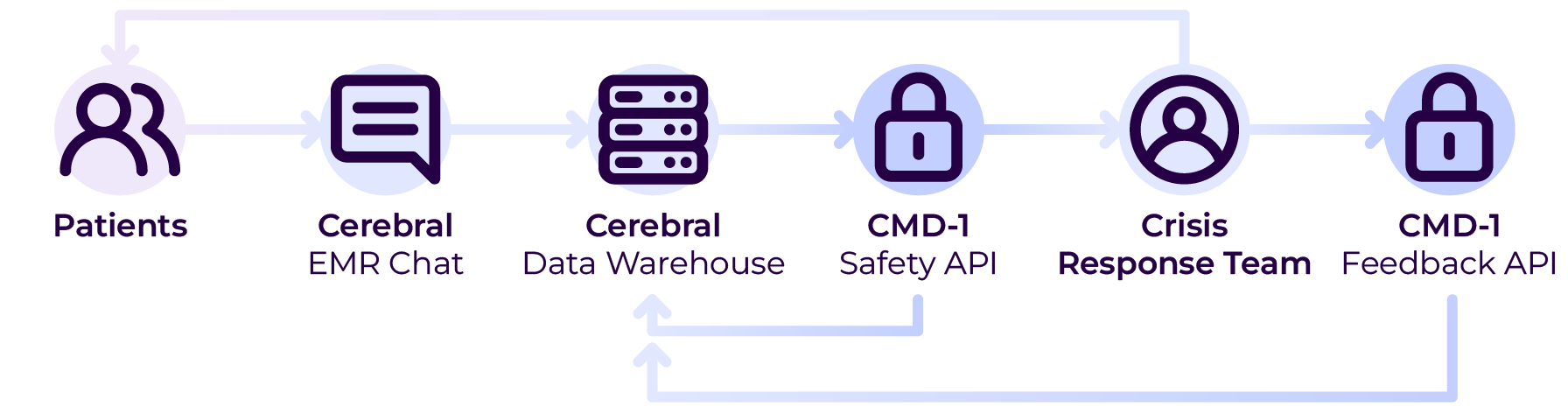
Figure 1. Overview of Crisis Message Detector-1 (CMD-1) System
CMD-1 is a tool that identifies messages from patients experiencing a mental health crisis and shares them with our crisis response specialists. It’s designed to alert the crisis response team to messages that may indicate suicidal ideation, homicidal ideation, non-suicidal self-injury, or domestic violence, among other emergency situations. Once alerted, the crisis response team reaches out to patients directly to assess the level of immediate risk, then mobilizes emergency contacts and/or local responders, if appropriate.
CMD-1 allows our care teams to significantly reduce the amount of time a patient experiencing a mental health crisis must wait before receiving support. During a week-long pilot, CMD-1 screened over 60,000 EMR messages and flagged more than 500 potential crises. The model successfully detected over 99% of all crisis messages and, as a result, crisis specialists were able to respond to patients in less than 9 minutes on average.
We are proud to have officially launched CMD-1 for all Cerebral patients, allowing our crisis specialists to support individuals when they are at their most vulnerable. This is just the beginning for machine learning-enabled solutions. In the coming months, we plan to apply this technology to improve response times for medication concerns, scheduling issues, and support requests across the board.
Special thanks to the Cerebral employees and advisors who participated in the design, build and testing of our CMD-1 System: Tyler Heist, Madeline Holmes, Matthew Rubashkin, Sid Salvi, Shaked Azzam, Dr. David Mou, Dr. Matthew Nock and the entire Cerebral Clinical Quality and Safety teams!


Using Data to Best Match Patients and Clinicians


Why Can’t We Talk About Suicide?


The State of Mental Health Care in 2022: Where are We?
Call 911 if you’re having a
mental health emergency
Text Home to 741-741 if you're in emotional
distress and need immediate support
Call or text 988 Suicide &
Crisis Lifeline. Chat service
is available at 988lifeline.org.